

It’s go time.
My awake craniotomy was scheduled for 8 am on September 9, 2015. I felt well prepared. I got up early, to take advantage of the last window for nourishment, at 5:30 am and downed a big cup of homemade bone broth. I scrubbed clean using the antiseptic sponges provided by the hospital, including my newly shaved head. I felt like a giant clean baby.
My husband and mother, sporting their freshly shaved heads in support, and my brother (the Barber, who already sported the look for years) drove me to my 6 am admission. The sun was rising as we travelled from our suburb through a quiet stretch of Saskatchewan prairie to the city, and I noted that we were all sporting grey toques. No plan at work there, but, hey. Greymadder in the house. Grey is the “cancer color” for brain tumours, for the same punny reason I coined my blog title, of course.
I am pleased to report that we “fed the calm” that morning, as prescribed in our preparatory planning. At least whatever nerves or doubts any of my posse had were held in check admirably.
I was reminded over and over that we can complain about shortfalls in our healthcare system, about staffing or infrastructure issues, about union and resource issues, but when it comes down to the wire, the people are amazing and do amazing work. And they are always passing out those heated cotton sheets. I mean, that’s just about the best thing ever.
Friends, if you’ve never had an awake craniotomy, buckle up. Here’s what it’s like. Or what mine was like, at least.
The surgical nurse (I never got her name, I regret that, she was awesome) brought me into the OR, and it was full of people. I was introduced, and my surgeon, Dr. F, made the formal announcement that today we were performing a stealth MRI guided awake craniotomy with functional brain mapping and tumour resection. That, together with the Sharpie marker signature he had written on the left top of my head in the holding area, gave me faith that I would avoid making the news as a medical error report.
I had already met the anaesthesiology resident, Dr. G, who would be running point, together with the anaesthesiology boss, Dr. D. They were both very confidence inspiring. They explained that once I was positioned for surgery, I would be able to hear everything, but only see one of them, who would be sitting in front of me at all times, an arm’s length away, and that my job was to simply tell him how I was feeling and if anything was uncomfortable or upsetting, they could “turn down the volume” on the experience. I asked if they could follow me around with that promise every day.
I climbed up onto the table (it seemed small), and Dr. G began setting up my IV, into an artery on the back of my right wrist. He showed me that they had a rack of three sedatives that they would be using in combination to manage that “experience volume”. He said that the baseline level of sedation they would be working to achieve would be relaxation, a feeling of peace where I may want to close my eyes, but would not sleep and would easily be able to respond if they said my name.
My surgeon, Dr. F, stepped behind me and told me he would start discussing positioning for surgery now. He had told me that the actual tumour removal wouldn’t take as much of the planned four hours as you might think, and that positioning, preparation and opening, then closing, takes up most of the time. There were surgical residents in the room, and also psychology department staff, who had run my functional MRI, and would be interested to see the brain mapping part of the operation and be able to compare the open brain data to what they had collected on fMRI. I recall Dr. F telling his folks that my neck was supple, so they had options for positioning, and because they were operating on the upper left part of the brain, he’d want the right side somewhat free for motor and sensory testing, so they would “airplane” the bed. That’s about the last I recall for a bit, as Dr. G had assured me that he would increase my sedation slightly during positioning (and catheter insertion, thanks Dr. G).
 The next thing I recall, I was aware that I’d been positioned, I was laying slightly on my right side, with both arms extended forward on an arm support. I could see clear plastic around my field of view (I was put in mind of my dog coming from the vet with the undignified cone). As promised, I could see Dr. G seated in front of me by my hands, and I could hear others going about their work. I was aware I was secured about the head and couldn’t move, but couldn’t really feel anything other than pressure. I distinctly remember feeling that something was going on with my legs, I apologized to Dr. G and asked him to let whoever was “in charge of my legs” know that I’m sorry, but I felt I needed to stretch my feet. I know know that I had a pump providing periodic compression to my lower legs, but I didn’t figure that out, I had the impression someone was down there massaging them or something. Like a spa.
The next thing I recall, I was aware that I’d been positioned, I was laying slightly on my right side, with both arms extended forward on an arm support. I could see clear plastic around my field of view (I was put in mind of my dog coming from the vet with the undignified cone). As promised, I could see Dr. G seated in front of me by my hands, and I could hear others going about their work. I was aware I was secured about the head and couldn’t move, but couldn’t really feel anything other than pressure. I distinctly remember feeling that something was going on with my legs, I apologized to Dr. G and asked him to let whoever was “in charge of my legs” know that I’m sorry, but I felt I needed to stretch my feet. I know know that I had a pump providing periodic compression to my lower legs, but I didn’t figure that out, I had the impression someone was down there massaging them or something. Like a spa.
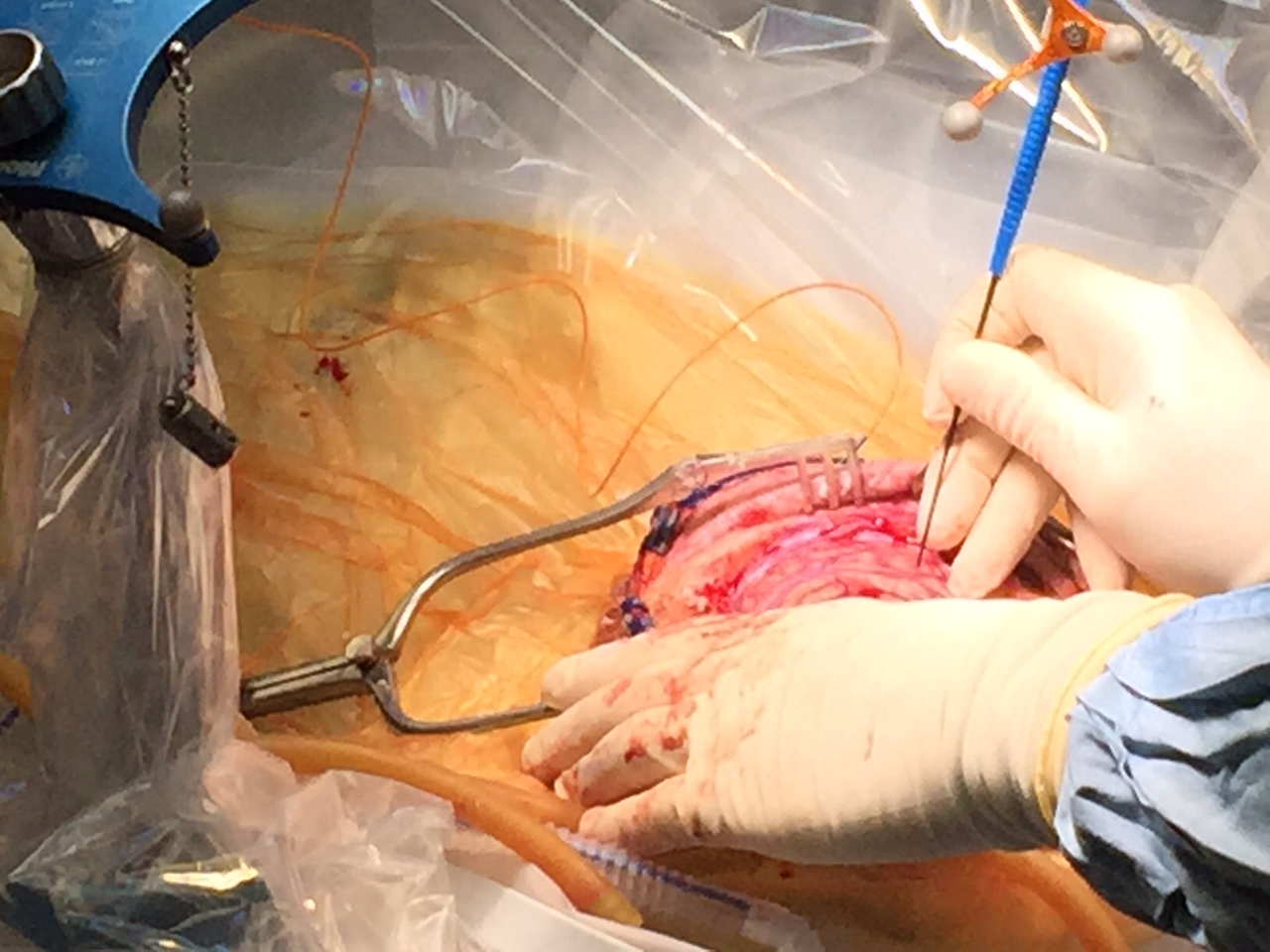
They told me they would now begin working on the incision, and that I may feel some pricks in my scalp from the local anaesthetic. I asked if anyone was taking photos. My surgeon said “well, we’re not set up for it, but I could get some on my cell phone if you want?” I said “yes, I want!”
Next steps are blurry, my reliable friend Dr. G turned down my volume I assume. I do recall the singular experience of realizing that I heard and felt the vibration of the saw. I called up my meditation target that I’d had prepared, and had some kind of out of body experience imaging my infinity walk while that sawing went on. I was aware of tears on my cheeks, though I could not feel any pain and didn’t feel anything akin to fear. I distinctly recall the feeling of Dr. G holding my hand at that point.
The next clear memory I have is of being called upon, “Alix, Alix?”. I said, “yes, yes, I’m here, I think I had a nap.” Dr. F told me it was time for me to do my job, and give them feedback on what I was feeling, because they were beginning the brain mapping part of the procedure. Here they probe areas of the brain that they’d imaged already using functional MRI, to assess motor and sensory function. Because my tumour was located right up against the motor sensory cortex, motor function was the primary concern. The fMRI had also shown some sensory response originating from within the tumour tissue, so determining whether that was a false positive image was on the list of to-do’s.
 I was asked to move my fingers, to touch both palms, and say whether anything felt different between them. This was repeated for my feet, move them, rub them together, report any tingling or sensations or anything different left side to right side. Dr. F asked me to continue to do that every 10 or 20 seconds. I think I took this job quite seriously. I have no recollection of feeling anything at all unusual. In retrospect, I find it amazing to believe that they could probe my motor cortex and elicit no effects at all. But if they did see any responses, I don’t remember it.
I was asked to move my fingers, to touch both palms, and say whether anything felt different between them. This was repeated for my feet, move them, rub them together, report any tingling or sensations or anything different left side to right side. Dr. F asked me to continue to do that every 10 or 20 seconds. I think I took this job quite seriously. I have no recollection of feeling anything at all unusual. In retrospect, I find it amazing to believe that they could probe my motor cortex and elicit no effects at all. But if they did see any responses, I don’t remember it.
I remember snippets of conversation between Dr. F and his resident, and the psychology department researchers, during this time. I know Dr. F concluded that there was no sensory response within the tumour tissue, and that imaging artifact was indeed a false positive. I remember he informed me that he was ready to perform the actual resection. He narrated that this was the advantage of an awake procedure, because he was confident in what he could remove and that he could remove more tissue than he might otherwise, because he could have my responses in real time. I listened to him teaching his assisting resident. I remember hearing “see, to me, that looks like tumour tissue, not healthy brain, look, do you see?” I remember Dr. F commenting that “the borders are really very well defined” on the tumour. I piped up with a ketogenic diet plug and offered to send him some references. I’m a smart ass, apparently, even sedated. He asked me to tell them again about the diet, and I obliged.
 I remember sometime in here complimenting my faithful Dr. G on his skill with the sedation; I informed him that I’d practiced up a great deal with a number of meditation targets, but that I was pleased to really not need them. I think he was amused, I was feeling very jovial. I gave up drinking when I was diagnosed three years ago; I was only ever good for one glass of wine anyway, so it was a small sacrifice. On that table, I felt a little like a college kid at a party, and I was confident I was the witty life of it.
I remember sometime in here complimenting my faithful Dr. G on his skill with the sedation; I informed him that I’d practiced up a great deal with a number of meditation targets, but that I was pleased to really not need them. I think he was amused, I was feeling very jovial. I gave up drinking when I was diagnosed three years ago; I was only ever good for one glass of wine anyway, so it was a small sacrifice. On that table, I felt a little like a college kid at a party, and I was confident I was the witty life of it.
Dr. F informed me “Alix, I want to tell you that I have removed everything I can see.” He is a pretty laid back guy, probably exactly what you want in a neurosurgeon. But at that point, he said “someone get me my cell phone, let’s call this lady’s husband.” There was a flurry of activity, they asked me the number and I called it out. Dr. G was passed the phone, and for a moment there was some doubt as to reception in the OR, and Dr. G offered to try from his phone. Then we heard my husband’s voice saying hello. Dr. G held the phone into me in my plastic cocoon, and Dr. F told me to tell him we got it all, and would be working on closing. My memory of what I said, confirmed later by my husband: “Dr. F says he got it all. Because he’s a rockstar, everyone in this room is a rockstar, and I’m a rockstar too. We have to go, he still has to close. I love you.”
 At that point, Dr. G asked if I was still needed, or if he should let me rest. Dr. F said “Alix’s work is done, but she seems to be doing fine, Alix?” I replied that I was good, so we chatted for what I take to be the 45 minutes or so that he was closing. He asked me about my company, what kind of research we do, and told me about a research project he had collaborated on with a private company. We talked about work and doing what you love. He said that he loves coming to work because he gets to do neurosurgery. He related a case where he’d done a similar resection years before, and how well the patient is doing now. He told me about what he expected next steps to be, in terms of getting pathology reports on the removed tissue, and reminded me that the fact that we’d seen growth could mean an advancement in staging of the tumour and that we’d need to be prepared for follow up treatments.
At that point, Dr. G asked if I was still needed, or if he should let me rest. Dr. F said “Alix’s work is done, but she seems to be doing fine, Alix?” I replied that I was good, so we chatted for what I take to be the 45 minutes or so that he was closing. He asked me about my company, what kind of research we do, and told me about a research project he had collaborated on with a private company. We talked about work and doing what you love. He said that he loves coming to work because he gets to do neurosurgery. He related a case where he’d done a similar resection years before, and how well the patient is doing now. He told me about what he expected next steps to be, in terms of getting pathology reports on the removed tissue, and reminded me that the fact that we’d seen growth could mean an advancement in staging of the tumour and that we’d need to be prepared for follow up treatments.
About that time, I became aware that there were staples going in my head. I needed the volume turned down on that.
Say what you want about supportive/alternative/complimentary medicine. This story right here is one of amazing medical science, technology, education and skill, at its finest. I am blessed and amazed to be somewhere this is available.
 Thank you to everyone who shared that experience with me.
Thank you to everyone who shared that experience with me.
Read on – Part III: Recovery and Release
Images courtesy of Dr. D. Fourney.
Added Oct 2, 2015 – here is a link to an interview with CBC Saskatoon on my diagnosis and surgery, live in studio from Oct 1.

rooting for you! ❤
LikeLike
Thank you very much!
LikeLike
” I remember Dr. F commenting that “the borders are really very well defined” on the tumour. I piped up with a ketogenic diet plug and offered to send him some references. I’m a smart ass, apparently, even sedated. He asked me to tell them again about the diet, and I obliged.”
You were right!!
And you brought me to tears when the Dr. F called your husband and you talked to him. Oh my.
LikeLike
I know, isn’t that amazing? It is an almost magical moment in my memory, definitely one of the high points of my life. That’s real caring medicine in action, in my opinion.
LikeLiked by 1 person
Alix, you’re so right: I tend to rail against modern medicine, but that’s mostly in regard to the ridiculousness that passes for diabetes care and education on the influence of diet on health. But when it comes to trauma and surgery, I have nothing but the utmost respect, awe, and gratitude for what medical doctors and modern technology are capable of. Sounds like you had a really fantastic team. And I guess we can’t say for certain whether the ketogenic diet helped the tumor stay well demarcated from the healthy tissue, but nor can we say for certain it *didn’t.* 😉 I think you’re absolutely right about the diet — it’s not a miracle cure, and anyone who claims it is, is on terribly shaky and dangerous ground. I think it can really help with quality of life and mitigating the side-effects of the conventional treatments, and I absolutely believe we need far more research on it than it’s currently getting in the cancer world. People should be given the relevant information so they can make an informed choice for themselves, but no one should be misled into thinking it’s a one-way ticket to being cancer-free. I try to make that clear in the blog series I’m doing about the metabolic theory of cancer.
These posts are wild! Thank you so much for sharing your experience with us.
LikeLike
Amy, yes. THIS.
Thank you so much for reading, I love your site and respect your opinion, thanks for your words. I have really relied on your blog and writing, it always seems you are on my wavelength. It can be difficult to strike the right tone between supportive, active, complementary things we can do, without running the risk of someone just reading one item and thinking their research is complete. I’ve struggled with that, and I really think you do a great job of addressing it. Thank you!
LikeLike
I’ve been following you for sometime now. I am writing through tears of joy for you. Best of luck (though you don’t need luck – but it’s what we say) with the remainder of your recovery.
LikeLiked by 1 person